Direct Primary Care makes complete sense as a concept. In the real world, of course, it’s a bit more messy and complicated, especially within the confines of an employer’s health plan, and finding the right pathway to achieve the desired results is sometimes tricky. Replacing the traditional entry point to a health care journey with a higher-performing primary care partner sounds ideal, up until the point when personal preferences and emotional bonds prove larger barriers than originally expected.
The main arguments against the traditional primary care pathway include:
- Providers get paid on a fee-for-service basis, so they are rewarded for managing chronic conditions and have no financial incentive for simply curing a condition.
- Primary care providers have to see too many patients in a day to meet the needs of a huge patient “panel.” Appointments are rushed, and rather than root-cause health care, only symptom-management is typically discussed.
- Primary care doctors often refer to specialists to protect from liability or malpractice claims.
- Upstream medical practices (i.e., more expensive providers such as hospitals) have purchased primary care providers to control the pathway to their services, and thus silently influence volume and referral patterns away from primary care treatment to their affiliated and more expensive providers and facilities.
The main value-propositions heralded by the DPC provider often include:
- Smaller patient “panels” equals more time spent with the patient (member).
- Money is spent to achieve wellness.
- Direct primary care is free from financial pressures and upstream interests.
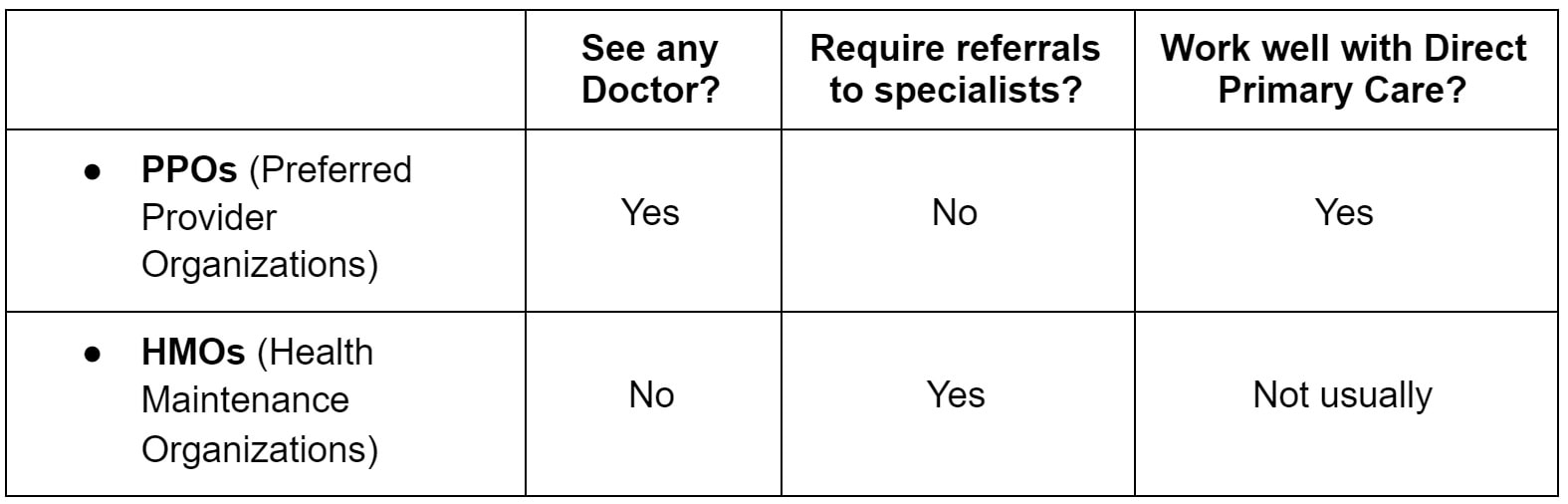
- The DPC model focuses on a broader scope of services and refers to specialists less often.
So, yes, it’s easy to see how the employer or consumer starts to recognize the advantages of this strategy. If the employer shifts their money from paying for services and instead moves that investment into a direct primary care relationship, their employees should get better care through a relationship with a provider who is compensated to focus more time on their employees and have fewer upstream referrals for testing and specialist interventions.
Built-in or bolt-on options for employers
There are several factors that determine whether the membership fees that a direct primary care practice receives are paid on an invoice basis to the employer, or whether their health plan administrator or TPA will make that payment.
Fully insured scenarios
The first and easiest distinction is the fully insured health insurance plan and its relationship to DPC practices. This one is simple: There isn’t a relationship. The DPC practice has rejected the traditional fully insured plan and built a practice where that relationship is predominately viewed as toxic and unhealthy for the patient and the provider. If an employer wants to establish a DPC relationship for their employees and the employees’ family members, this is a “bolt-on” option. The employer will either pay a monthly invoice for the membership fees, or the employees will pay directly and get a reimbursement from their employer.
Now, if you’re wondering, “Why would an employer pay extra for a DPC membership on top of their high-cost health care?” you are not alone.
I asked Dr. James Pinckney of Diamond Physicians in Dallas about this during my very early investigation into DPC in my local community. His response was simple: It’s about access and providing a huge benefit. His clients who were doing this were looking to provide an unparalleled benefit, and this was a simple way to do so while showing interest in the wellness aspect of their employees’ lives through the DPC memberships.
Most brokers I’ve spoken with who have this arrangement often use a high-deductible plan as the insurance vehicle for these arrangements, either because they need to save some money on the insurance to finance the DPC investment, or because the client already had an HDHP and needed to find a solution to address the perceived barrier to care that the health plan’s deductible was creating in the minds of their employees.
Self-insured or level-funded scenarios
The self-insured health plan is a much easier vehicle to customize with a built-in DPC option. When working with a plan’s administrator, you can typically arrange a per member per month fee to be invoiced to the employer and then submitted to the DPC practice, or you can define how the membership will be paid from the plan’s claims funds each month.
Of course, the real world is more complex than that made it sound.
Not all self-funded or level-funded plan administrators are adaptable. Some will simply have a set number of plan designs and pre-set protocols that they can’t and shouldn’t deviate from due to their operations. Others will give great lip-service to the concept and promise to accommodate, then utterly fail when it comes to execution or implementation.
To be fair, this is still a new process and hasn’t yet been adopted by the masses. Thus, most are learning with us as we go. And a plan administrator that can’t coordinate the monthly membership fees shouldn’t be a deal-breaker. Most DPC practices actually prefer to receive their payments directly from the employer group. Running a DPC arrangement as a bolt-on solution is not a horrible outcome, even with a self-funded plan.
I talked to Josh Butler of Butler Benefits about his experience with the bolt-on approach as the purest relationship for the employer and the DPC practice. “I’ve seen two mindsets from our employers. They either want to work directly with the DPC providers and form a deeper partnership with them, or they want to see the health plan take care of the tactical aspects of the provider relationship.” When I asked him which he saw driving better results, he said, “What kind of question is that? You know the employer that gets their hands dirty finds the gold.”
But, there is still great upside potential in the self- and level-funded arenas for the DPC arrangement to take hold and multiply.
For one thing, upfront cost reductions are possible here. Some stop-loss vendors will give discounts for a plan that uses a DPC solution. I’ve seen quotes that reduced insurance costs in the $25 to $40 per member per month range, and I’ve heard from peers about even higher per employee savings.
Coupling this fixed cost savings with the plan’s year-round performance through reduced upstream costs each time a member avoids unnecessary or overpriced care should be sweet music to the employer’s ears.
Prescription costs are another area of concern for the self-funded health plan, and monitoring the prescription usage before and after implementing a DPC strategy can help shed light on the greater potential of this relationship. Prescription usage will obviously be a slower impact item, but having that higher engagement and the anecdotal data that most DPCs gather after blunt conversations about the cost of care and the cost of prescriptions will inevitably begin to assist the plan’s performance in this area.
Preparing for the complex scenarios
Inevitably, the actual implementation will be some variation or expansion on the simple DPC arrangement. There will be an adjustment to the concept based on discussions that arise with the employer and their leadership team. There will also likely be adjustments once all parties review prices from various DPC vendors and after employees provide their feedback.
More than one DPC vendor
You will need to be prepared to address the impact of geographical regions, which could include discussing a 20-minute drive across one city, a two-hour commute between different counties in the same state, or even coverage across multiple states.
Some DPC practices have grown their own geographical footprints to meet the needs of the customers they currently serve through hiring; some of those practices will also extend their billing and administrative services to other independent DPC practices to create a seamless experience for the employer group, while not having to own and staff a new region.
And there are software services that can leverage existing relationships to create custom networks of DPC practices. These services have really started refining their deployment, and while these services typically add expense to the setup and administration, the flexibility for a multi-location employer to deploy a DPC solution without spending the time to create individual relationships or band-aid geographic holes can be a huge value for the right clients.
Sharing DPC costs with the employee
This is where we come back to the built-in or bolt-on conversation. This is really a moot point in the built-in scenario when the plan or TPA administers the membership fees, and the employer has bundled everything into the traditional payroll deduction scenario. But, in the “bolt-on” or separate enrollment and billing scenario, things get more interesting.
Tom DiLiegro of Benefits Advisors of South Charleston has seen the full spectrum. “When the employer understands the impact and the savings at stake, they immediately want to pay for the membership fees in full. Once they start to consider employees who don’t go for routine care today, they start down the slippery slope of not wanting to pay for medical care on behalf of employees who don’t receive care today. Inevitably, they end up with a 75%/25% cost-sharing or 100% cost-sharing for a limited time, but then reduce or remove the employer portion of the DPC for those employees who don’t have their first visit within a set number of months into the new DPC arrangement.”
DPC and VDPC options and combinations
All DPCs have virtual care covered in their memberships; that is one of their main value propositions. Some even give price breaks for a virtual-only membership. But the emergence of 100% virtual primary care practices and the expansion of services offered by telemedicine solutions is going to be central to any DPC conversation.
My personal experience has been predominantly with the DPC/VDPC combination using two different vendors. The structure is to use a DPC for those in a reasonable geographical location, and a virtual-only vendor for employees who live in a region without a feasible DPC relationship, or a region without enough employees to establish a company-paid membership with a DPC provider. This isn’t always the solution that the DPC partner prefers, but the price point on these arrangements is often more palatable for the employer groups and the VDPC vendors are often easier for the employer to deploy.
Sherpaa founder and CEO Jay Parkinson’s prediction that care will be “primarily online and strategically in person” is increasingly likely and occurring a little quicker than even he expected when he offered this as a central theme to a talk he delivered in February 2020.
Worth it?
So many hurdles, shifting scenarios, and uncertainties beg the question: Are the results worth the time, effort and money?
This is about a journey in pursuit of a different result. When an employer, advisor or individual wants a reset on their health care expenditure, they need to try a new path. Whether the first step is a DPC arrangement, a virtual DPC, or even contracting directly with a traditional practice willing to perform in a more attentive and high-value manner similar to the ACO model, a new pathway that starts with primary care is a sensible place to start.
Savings might occur immediately, in year three, or might never be realized, but anything strategically done to lower costs and improve the health of a workforce has to be considered worthwhile.
Want to learn more about Direct Primary Care for your business? Visit our dedicated employer page - www.HealthcareforJax.com
- Article from Benefits Pro 4/7/21 -Bret Brummitt is a benefits consultant and the founder of Generous Benefits.